
Research ArticleOpen Access, Volume 4 Issue 1
Perception of workplace violence risk among healthcare workers: A single center cross-sectional survey
Giovanna Sepe1*; Giovanni Cirillo2
1Direzione Sanitaria OO.RR. Area Nolana, ASL NA3 Sud, Italy.
2Department of Mental and Physical Health and Preventive Medicine, University of Campania “Luigi Vanvitelli, Naples, Italy.
*Corresponding author: Giovanna Sepe
Direzione Sanitaria OO.RR. Area Nolana, ASL NA3 Sud, Via Seminario, 80035 Nola (NA), Italy.
Email: gi.sepe@aslnapoli3sud.it
Received : Nov 05, 2025 Accepted : Feb 03, 2026 Published : Feb 10, 2026
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Sepe G © All rights are reserved
Citation: : Sepe G, Cirillo G. Perception of workplace violence risk among healthcare workers: A single center cross sectional survey. Epidemiol Public Health. 2026; 4(1): 1086.
Abstract
Objective: Workplace Violence (WPV) is an increasing concern in healthcare. This study investigated the perception of WPV risk among healthcare professionals at Nola Hospital, Southern Italy, in 2023, focusing on awareness, contributing factors, and preparedness.
Methods: A structured questionnaire with closed- and open-ended questions was administered to staff. Sixty-five responses were collected and analyzed descriptively.
Results: Although 90.8% of respondents do not usually work alone, 27.8% perceive their workplace as unsafe. Most (66.7%) consider WPV risk measurable, and 70.8% identify key contributing factors such as long waiting times, understaffing, and poor communication. Only a minority reported receiving training. Open responses emphasized distress, under resourcing, lack of procedures, and a culture of silence.
Conclusion: Findings reveal a gap between staff awareness and institutional preparedness, underscoring the need for structured protocols, training, and a culture of safety.
Keywords: Workplace violence; Healthcare workers; Risk perception; Occupational safety; Hospital-based survey.
Introduction
Workplace Violence (WPV) in healthcare settings has emerged as a critical issue for health systems globally, repre senting a growing threat to the safety, dignity, and psychologi cal well-being of healthcare workers [1,2]. Defined by the World Health Organization as “incidents where staff are abused, threatened or assaulted in circumstances related to their work” [3], WPV encompasses verbal abuse, physical aggression, threats, and in some cases, severe traumatic experiences. Hos pitals—especially emergency departments, psychiatric units, and outpatient clinics—are among the most frequent scenarios in which such violence unfolds [3,4].
Healthcare professionals are uniquely vulnerable to WPV due to a combination of environmental, organizational, and interpersonal factors [5]. These include overcrowded and un derstaffed wards, long waiting times, emotionally charged in teractions, mental health comorbidities among patients, and systemic stressors within public health services [6]. In Italy, the phenomenon has been increasingly reported in both national statistics and anecdotal evidence, yet remains under-recog nized and under-reported due to stigma, fear of retaliation, and normalization of violence as “part of the job”[7].
Although legislative efforts have been made to protect healthcare workers (such as Law 113/2020, which introduces stricter penalties for assaulting healthcare personnel), imple mentation and prevention strategies remain uneven across regions. The Campania region, in particular, has been the fo cus of attention due to repeated episodes of violence against healthcare staff reported in both media and internal reports [8]. Nevertheless, a structured understanding of how healthcare workers perceive and experience WPV, and whether they feel adequately prepared to address it, is still lacking.
Perception plays a pivotal role in the risk management framework of WPV: while objective indicators of violence (e.g., number of reported assaults, injuries) are essential, subjective elements such as perceived safety, confidence in institutional support, and emotional response to risk are equally important for designing effective interventions. Previous research shows that when healthcare workers perceive their environment as unsafe or unpredictable, their job satisfaction, mental health, and performance are significantly compromised [9,10]. More over, the availability of training and clear institutional proce dures has been associated with greater resilience and a lower incidence of aggression-related burnout [11]. However, in many Italian hospitals, training programs on de-escalation techniques and conflict management are inconsistently delivered or entire ly absent. As a result, healthcare workers often rely on personal coping mechanisms, which may be insufficient and potentially harmful in the long term.
In this context, the present study aims to investigate the per ception of workplace violence among healthcare professionals at the “Ospedale Santa Maria della Pietà” in Nola (Italy). The hospital, located in a densely populated area of the Naples met ropolitan region, serves a large and socioeconomically diverse patient population, often under conditions of structural and staffing limitations. As such, it provides a meaningful setting to explore both individual awareness and systemic preparedness regarding WPV. The study utilizes a structured questionnaire composed of quantitative and qualitative elements, adminis tered to a representative sample of hospital staff. The survey explores four main domains: (1) the perception of safety and risk of aggression; (2) knowledge of contributing factors; (3) personal experience with violence and emotional consequenc es; and (4) awareness of and access to institutional tools, such as training or protocols. Open-ended questions further enable participants to express concerns or suggestions that may not be captured in closed formats.
The research is motivated by both scientific and operational objectives. Scientifically, it contributes to the sparse literature on WPV in Southern Italian healthcare contexts, where regional disparities in resource allocation, staffing, and organizational cul ture can significantly shape experiences of violence. Operation ally, the findings aim to inform local policy development, training programs, and risk management strategies at the institutional level. Understanding how healthcare workers perceive and inter pret WPV risk is essential not only to address current vulnerabil ities, but also to build a proactive culture of safety and resilience.
The present study also aligns with international calls for healthcare systems to recognize WPV not as an occasional or unavoidable phenomenon, but as a structural and preventable hazard. By prioritizing healthcare worker safety, institutions in directly improve patient outcomes, staff retention, and overall quality of care [12]. In an era marked by increasing pressures on public health services, investing in workplace safety is not a luxury, but a necessity.
Materials and methods
Study design and setting
This study employed a cross-sectional, observational design based on a structured questionnaire administered at the “Os pedale Santa Maria della Pietà” in Nola (Italy) in 2023. The hospi tal is a public, medium-sized acute care facility serving a densely populated and socioeconomically diverse area, with an elevat ed patient throughput and high-pressure clinical environments such as emergency medicine, internal medicine, and pediatrics.
Participants and sampling
The target population consisted of healthcare workers em ployed in the hospital at the time of the study, including phy sicians, nurses, and allied health professionals. A total of 65 respondents completed the questionnaire voluntarily and anonymously. Inclusion criteria were current employment at the hospital, direct involvement in patient care, and consent to participate. No financial or institutional incentives were offered. Due to the exploratory nature of the study, no formal power calculation was performed; the sample was intended to provide a snapshot of risk perception across professional roles and de partments.
Instrument
The questionnaire was developed based on national and international literature on workplace violence in healthcare [3,7] and reviewed for face validity by a panel of three senior clinicians and a hospital risk manager. It included closed-ended questions (yes/no and multiple choice) to assess frequency and type of exposure to violence, perceived safety, and knowledge of risk factors, as well as open-ended items to collect qualitative insights into personal experiences and institutional challenges.
The survey consisted of 25 items grouped into four thematic sections:
1. Perception of safety and isolation at work;
2. Awareness of WPV and contributing factors;
3. Knowledge of definitions, reporting, and institutional support;
4. Free-text responses on perceived causes, personal experiences, and suggestions.
The questionnaire was distributed in paper format during departmental meetings and collected in sealed envelopes to ensure confidentiality.
Data analysis
Quantitative data from closed-ended responses were en tered into a Microsoft Excel database and analyzed using de scriptive statistics. Frequencies and percentages were calcu lated for each item (e.g., proportion of respondents who report working alone, perception of environmental safety, awareness of violence definitions). Due to the relatively small sample size, no inferential statistics were applied.
Qualitative data from open-ended responses were analyzed thematically using a manual content analysis approach. Two independent researchers reviewed all text entries and catego rized them into recurring themes and subthemes. Discrepancies were resolved through discussion, and representative quotes were extracted to illustrate common viewpoints and concerns. Categories included: perceived causes of violence (e.g., long waiting times, understaffing), emotional responses (e.g., fear, frustration), and perceived institutional shortcomings (e.g., lack of training, unclear procedures). Data triangulation between closed and open-ended items allowed for a deeper understand ing of how perceived risk aligns with structural factors and emo tional responses.
Ethical considerations
Participation in the survey was entirely voluntary, anony mous, and conducted in accordance with the ethical standards of the institutional risk management office. The questionnaire did not collect any personal identifiers. Participants were in formed of the purpose of the study, and data were processed in compliance with Italian data protection regulations (EU GDPR 2016/679). Given the non-interventional nature of the survey and the absence of sensitive clinical data, formal ethics commit tee approval was not required under Italian law.
Results
Respondent demographics and general context
A total of 65 healthcare workers participated in the survey conducted at “Ospedale Santa Maria della Pietà” in Nola (Italy). Although no personal demographic data were collected to pre serve anonymity, respondents included a heterogeneous group of clinical professionals, primarily physicians, nurses, and allied health staff. All participants were actively engaged in direct pa tient care. The majority reported regular shifts in emergency, medical, surgical, pediatric, or outpatient services.
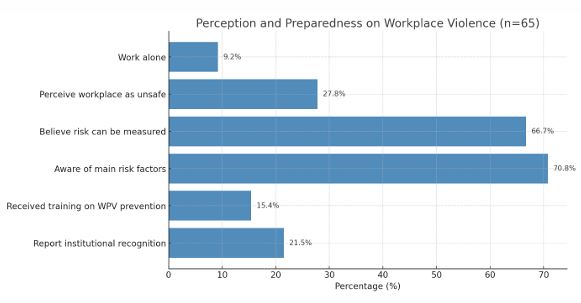
The purpose of the questionnaire was to assess perceived risk of workplace violence, knowledge of contributing factors, emotional reactions, and perceived adequacy of institutional support. The results reflect both measurable gaps in prepared ness and significant emotional and cognitive engagement with the issue of violence in clinical settings (Figure 1).
Working conditions and perceived safety
Only 6 out of 65 respondents (9.2%) indicated that they habitually work alone, whereas the overwhelming majority (90.8%) reported working in team-based settings. Despite this, a considerable 27.8% (18 respondents) expressed the belief that the workplace is not safe. This dissonance suggests that the perception of safety is not solely related to physical isola tion, but rather to systemic vulnerabilities and a lack of support structures. Qualitative responses reinforced this interpretation, with multiple participants referring to “chaotic working condi tions,” “lack of control in emergency settings,” and a general sense of “institutional indifference”. One nurse wrote, “We are not alone physically, but we feel abandoned when violence oc curs—there is no protocol, no one to protect us.”
Awareness and definitions of violence
Participants were asked whether they could define work place violence. While the question was open-ended and re sponses varied, the majority associated violence with both ver bal and physical aggression, extending from patients and their families toward clinical staff. Several definitions included emotional abuse and threats, indicating a broad understand ing of the concept. Among those who elaborated in open text, many cited past experiences: “I consider it violence when a family member yells in your face for a delay that is not your fault,” or “Physical aggression is rare, but psychological pres sure is constant.” These insights reveal that healthcare workers experience violence as a spectrum, often beginning with subtle verbal hostilities that escalate if unaddressed.
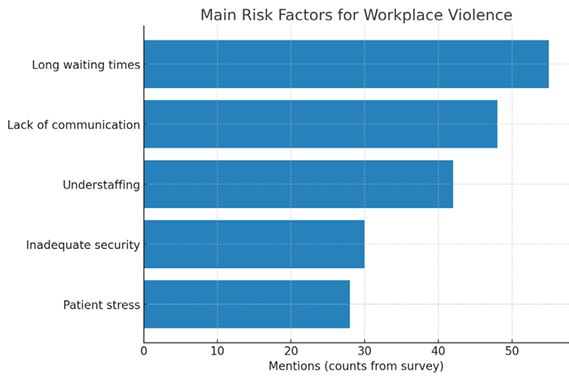
Measurability and risk factors
To the question, “Can the risk of violence be measured?” 46 out of 69 responses (66.7%) answered affirmatively. This sug gests an intuitive understanding among staff that certain envi ronments, times of day, and patient profiles are associated with higher risk. In the multiple-choice section asking about specific risk factors (Figure 2), respondents identified:
• Prolonged waiting times
• Lack of communication with users
• Understaffing
• Inadequate security personnel
• High stress among patients and caregivers
One participant emphasized: “The aggression is a conse quence of a system that is constantly in emergency mode. Pa tients wait for hours without explanations, and that fuels anger.” Another wrote: “Violence is the result of broken expectations. People think hospitals should solve everything instantly.” Such responses underscore the connection between systemic inef ficiencies and individual risk perception. Notably, very few par ticipants attributed violence to “pathological” behavior alone, indicating a broader socio-organizational understanding of the phenomenon.
Institutional awareness and training
When asked whether violence is recognized at the institu tional level, only 14 out of 65 participants (21.5%) responded af firmatively, suggesting a deep-seated skepticism among staff re garding the hospital’s readiness or willingness to address WPV structurally. Further, only 10 respondents (15.4%) reported having received formal training on how to prevent or manage workplace violence. Several participants noted that even when training was available, it was general and theoretical, with no follow-up simulations or practical guidance. A physician not ed: “We were shown a slide presentation years ago, but there is no system in place. It’s forgotten the moment it’s over.”
The absence of a dedicated emergency protocol or reporting mechanism was cited repeatedly as a barrier to prevention. Re spondents emphasized the lack of clear pathways for reporting incidents or seeking support after a traumatic event.
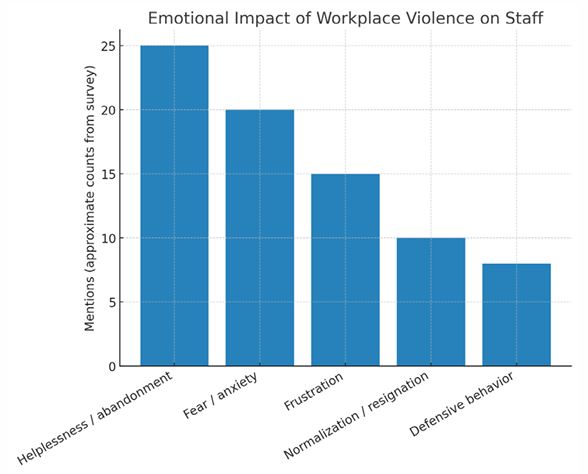
Emotional impact and psychological consequences
Open-ended responses provided powerful insight into the psychological toll of WPV (Figure 3). A recurring theme was the normalization of aggression: “You get used to it, or you quit.” Others described feelings of helplessness and isola tion: “You report something, and no one follows up,” and “We are treated as if we provoked the aggression ourselves.”
Several participants mentioned changes in their clinical be havior due to fear: avoiding eye contact, minimizing explana tions, or rushing patient interactions to avoid potential escala tion. One nurse wrote, “I stopped working night shifts because I’m afraid to be alone with angry relatives.”
These narratives align with literature on the emotional blunt ing, defensive practice, and burnout that frequently result from unmanaged exposure to workplace violence [11,13].
Suggestions for improvement
The final section of the questionnaire invited suggestions for institutional improvement. Recommendations included:
• Mandatory de-escalation training;
• Presence of security guards in critical areas;
• Post-incident psychological support;• Post-incident psychological support;
• Clear incident-reporting procedures;
• Transparent communication with users.
A participant summarized: “What we need is not only pun ishment for aggressors, but protection and recognition for us.”
Others called for public awareness campaigns, both to sup port healthcare staff and to re-establish respectful relationships between institutions and the communities they serve.
Results
In summary, these data reveal a highly aware but insuffi ciently supported workforce. Healthcare workers at Nola Hospi tal perceive workplace violence as a frequent and multifactorial risk, rooted not only in individual behavior but also in systemic dysfunction. While most staff can recognize risk factors and de scribe personal experiences of violence, they report a lack of institutional training, protocols, and follow-up support. Emo tional exhaustion, resignation, and defensive clinical behavior were common themes in open-ended responses. Together, these findings point to an urgent need for structured interven tion and cultural change.
Discussion
This study offers a detailed snapshot of how healthcare pro fessionals at “Ospedale Santa Maria della Pietà” in Nola (Italy) perceive the risk of workplace violence, interpret its causes, and evaluate the institutional capacity to prevent and respond to such incidents. The results point to a workforce that is both highly aware of the phenomenon and deeply disillusioned by the lack of systemic support. These findings echo internation al literature [14] while adding region-specific insight into the structural vulnerabilities of the Italian public health system, par ticularly in high-pressure environments such as Southern Italy.
The reported prevalence of perceived workplace violence risk—nearly one in three respondents declaring their workplace as unsafe—is consistent with global studies identifying health care as one of the most violence-prone occupational sectors [10,15]. However, unlike many large-scale epidemiological sur veys that focus on incident frequency or injury rates, this study emphasizes perceived safety, a subjective but highly informa tive measure of risk that strongly correlates with burnout, ab senteeism, and intention to leave the profession [16].
A particularly significant result is the fact that only 15% of respondents reported receiving any form of training in violence prevention or de-escalation. This mirrors findings from other Italian and European studies suggesting that WPV remains poorly integrated into institutional training curricula, especially outside psychiatric and emergency contexts [17]. The lack of preparedness is compounded by the absence of clear protocols, which many participants identified as a key barrier to reporting and resolving incidents. As previously reported [18], merely ac knowledging the existence of violence is insufficient; proactive systems must be put in place to monitor, respond, and follow up on aggression toward healthcare workers.
One of the major strengths of the study lies in its explora tion of qualitative responses, which illustrate the multifacto rial nature of violence. Most respondents recognized systemic factors—such as long waiting times, understaffing, and poor communication—as more influential than individual pathol ogy in provoking aggression. This view is supported by multiple studies identifying organizational inefficiencies as primary risk amplifiers [4,6]. The implication is clear: violence should not be interpreted merely as a result of patient frustration or men tal illness but as a predictable consequence of service delivery breakdowns.
The fact that most staff did not work alone, yet still felt un safe, suggests that physical presence is not sufficient protec tion in the absence of coordinated institutional support. Feeling “alone” in the face of violence—psychologically and procedur ally—emerges as a recurring theme. This aligns with theories of institutional betrayal, where organizations fail to protect their employees or to acknowledge their suffering [19]. The emotion al burden described by participants—ranging from frustration to resignation and fear—reflects the psychological toll of sus tained exposure to aggression. The findings mirror international evidence linking WPV to increased rates of emotional exhaus tion, sleep disturbances, PTSD-like symptoms, and diminished professional engagement [12,13]. Perhaps more alarmingly, several respondents reported changes in clinical behavior aimed at minimizing exposure to conflict—shortening explanations, avoiding eye contact, or refusing night shifts. These are classic markers of defensive medicine and emotional withdrawal, both of which degrade the quality of care and increase the risk of errors [20]. They also have implications for patient satisfaction and institutional trust.
A recurring concern in the responses is the institutional si lence surrounding WPV. Several participants felt that reporting would not result in any meaningful action and that aggression was normalized as part of the job. This phenomenon has been described in multiple healthcare systems, where under-report ing stems not only from bureaucratic barriers but also from a deeply rooted cultural acceptance of abuse as “inevitable” [18,21].
Changing this culture requires more than protocols; it re quires visible leadership, clear consequences for aggression, and positive reinforcement for reporting. As indicated by Leape and colleagues [22], transforming institutional culture around safety must begin with psychological safety—a shared belief that one can speak up about risks and violations without fear of blame or retaliation.
The study’s setting in the Campania region adds a critical dimension. Southern Italian hospitals face persistent resource constraints, higher patient volumes, and complex social dynam ics, all of which increase the baseline risk of violence. While re cent Italian legislation (Law 113/2020) has strengthened legal protections for healthcare workers in Italy, its implementation remains uneven, particularly in resource-poor contexts. There is often a disconnect between normative frameworks and on-the ground enforcement. This gap is not unique to Italy: a WHO re view [23] identified similar barriers in multiple health systems: lack of data collection, minimal inter-sectoral coordination, and limited financial investment in staff protection. However, the Italian context is particularly fragile due to political fragmenta tion and chronic underfunding in certain regions.
Limitations
This study has several limitations. First, the sample size, al though adequate for descriptive analysis, limits generalizability and precludes inferential statistical testing. Second, the absence of demographic data—though intentional to preserve anonym ity—prevents analysis by profession, department, or years of experience. Third, the self-reported nature of the survey may introduce bias, particularly in underreporting of violence due to internalized stigma or fear of reprisal.
Despite these limitations, the study provides rich, actionable insight into the lived experience of healthcare workers facing WPV in a real-world clinical environment.
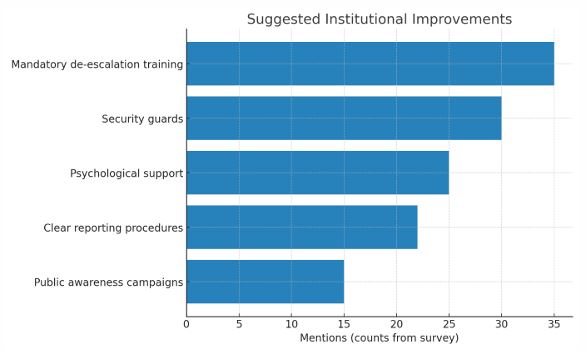
The findings suggest several concrete actions (Figure 4):
Mandatory training on violence prevention and de-escala tion techniques, integrated into professional development pro grams, as also previously indicated [24].
Clear institutional protocols for managing WPV incidents, in cluding incident reporting, documentation, and follow-up sup port.
1. Staffing improvements, particularly during high-risk periods (e.g., night shifts, emergency overflow).
2. Public awareness campaigns to educate patients and families about healthcare processes and mutual respect.
3. Psychological support systems, including post-incident counseling and peer support networks.
Additionally, the hospital leadership must commit to a vis ible cultural shift, actively condemning violence, supporting af fected staff, and creating safe avenues for reporting.
In conclusion, WPV in healthcare is not an isolated event but a structural vulnerability that threatens staff well-being and patient safety alike. At Nola Hospital, as in many similar insti tutions, healthcare professionals possess a clear and nuanced understanding of the phenomenon. However, without insti tutional recognition, adequate training, and clear operational frameworks, this knowledge remains an unutilized resource. By integrating the voices and experiences of frontline workers into policy and training, institutions can move from passive toler ance to active prevention. Addressing WPV is not just a matter of legal compliance or reputation management; it is a founda tional step toward building resilient, ethical, and safe health care systems.
Learning outcomes
• At the end of this article, readers will be able to identify measurable risk factors for workplace violence in healthcare, including understaffing, long waiting times, and poor communication.
• Readers will recognize the gap between staff awareness and institutional preparedness, highlighting the need for structured protocols and mandatory training.
• Readers will be able to apply findings to develop time-bound interventions that improve staff safety, reduce burnout, and enhance patient care quality.
Declarations
Acknowledgments: Authors thank all colleagues and healthcare workers who gave their time and consent to this work.
Author contributions: GS: study conception and design; data acquisition, analysis, interpretation, drafting/revising the article; approval of the final version. GC: data analysis and interpretation; drafting/revising the article; approval of the final version.
Data availability: The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
AI detailed statements: NO AI was utilized at any stage during research development & design, data collection, and manuscript preparation.
Ethical considerations & disclosure(s): Participants gave their consent to participate anonymously.
References
- Lim MC, Jeffree MS, Saupin SS, Giloi N, Lukman KA. Workplace violence in healthcare settings: the risk factors, implications and collaborative preventive measures. Ann Med Surg. 2022; 78.
- Kumar RP, Verghese W, Hegde D, Rasquinha SL, Rao RM, Kumar A. Workplace violence in the healthcare setting and its psychological impact on healthcare workers. Ind Psychiatry J. 2025; 34: 45–52.
- ILO, ICN, WHO, PSI. Framework guidelines for addressing workplace violence in the health sector. ILO/ICN/WHO/PSI Joint Programme on Workplace Violence in the Health Sector.
- D’Ettorre G, Pellicani V, Mazzotta M, Vullo A. Preventing and managing workplace violence against healthcare workers in Emergency Departments. Acta Biomed. 2018; 89: 28–36.
- Rossi MF, Beccia F, Cittadini F, et al. Workplace violence against healthcare workers: an umbrella review of systematic reviews and meta-analyses. Public Health. 2023; 221: 50–59.
- Pompeii LA, Schoenfisch AL, Lipscomb HJ, Dement JM, Smith CD, Upadhyaya M. Physical assault, physical threat, and verbal abuse perpetrated against hospital workers by patients or visitors in six U.S. hospitals. Am J Ind Med. 2015; 58: 1194–1204.
- Magnavita N. Workplace violence and occupational stress in healthcare workers: a chicken-and-egg situation—results of a 6-year follow-up study. J Nurs Scholarsh. 2014; 46: 366–76.
- Ministero della Salute. Relazione annuale sulla violenza contro gli operatori sanitari. Direzione Generale della Prevenzione Sanitaria.
- Gacki-Smith J, Juarez AM, Boyett L, Homeyer C, Robinson L, MacLean SL. Violence against nurses working in US emergency departments. J Nurs Adm. 2009; 39: 340–49.
- Spector PE, Zhou ZE, Che XX. Nurse exposure to physical and nonphysical violence, bullying, and sexual harassment: a quantitative review. Int J Nurs Stud. 2014; 51: 72–84.
- Lanctôt N, Guay S. The aftermath of workplace violence among healthcare workers: a systematic literature review of the consequences. Aggress Violent Behav. 2014; 19: 492–501.
- LeBlanc MM, Kelloway EK. Predictors and outcomes of workplace violence and aggression. J Appl Psychol. 2002; 87: 444–53.
- Gates DM, Gillespie GL, Succop P. Violence against nurses and its impact on stress and productivity. Nurs Econ. 2011; 29: 59–66.
- Leźnicka MM, Zielińska-Więczkowska H. Violence in the workplace: the occurrence of the phenomenon in relation to health care workers. Psychiatr Pol. 2024; 58: 351–62.
- Zhao S, Xie F, Wang J, et al. Prevalence of workplace violence against Chinese nurses and its association with mental health: a cross-sectional survey. Arch Psychiatr Nurs. 2018; 32: 242–47.
- Tsukamoto SAS, Galdino MJQ, Barreto MFC, Martins JT. Burnout syndrome and workplace violence among nursing staff: a cross-sectional study. Sao Paulo Med J. 2022; 140: 101–07.
- Magnavita N, Heponiemi T. Workplace violence against nursing students and nurses: an Italian experience. J Nurs Scholarsh. 2011; 43: 203–10.
- Arnetz JE, Hamblin L, Ager J, et al. Underreporting of workplace violence. Workplace Health Saf. 2015; 63: 200–10.
- Smith CP, Freyd JJ. Institutional betrayal. Am Psychol. 2014; 69: 575–87.
- Winstanley S, Whittington R. Aggression towards health care staff in a UK general hospital: variation among professions and departments. J Clin Nurs. 2004; 13: 3–10.
- Pich J, Hazelton M, Sundin D, Kable A. Patient-related violence against emergency department nurses. Nurs Health Sci. 2010; 12: 268–74.
- Leape LL, Shore MF, Dienstag JL, et al. A culture of respect, part 1: the nature and causes of disrespectful behavior by physicians. Acad Med. 2012; 87: 845–52.
- World Health Organization. Barriers in health systems: lack of data collection, minimal inter-sectoral coordination, and limited financial investment in staff protection. World Health Organization.
- Geoffrion S, Hills DJ, Ross HM, et al. Education and training for preventing and minimizing workplace aggression directed toward healthcare workers. Cochrane Database Syst Rev. 2020.