
Research ArticleOpen Access, Volume 4 Issue 2
Adherence to Community-Acquired Pneumonia (CAP) management protocol among hospitalized patients: A retrospective analysis
Ahmad Subhi1*; Salma Alshamsi1; Sarah Al-Toubah3; Afra Khan3; Anisha Paul3; Fardeen Mohammad3; Reem Sadeq3; Mohammed Alsuraihi5; Aulin Vitus2
1Department of Medicine, Adult Infectious Disease, Al-Qassimi Hospital, Sharjah, UAE.
2Department of Prevention and Control of Infection, Al-Qassimi Hospital, Sharjah, UAE.
3Department of Internal Medicine, Al-Qasimi Hospital, Sharjah, UAE.
4Intern, Al-Qasimi Hospital, Sharjah, UAE.
5Medical Student, Department of Medicine, University of Sharjah, Al-Qasimi Hospital, Sharjah, ARE.
*Corresponding author: Ahmad Subhi
Adult Infectious Disease, Department of Medicine, Al-Qassimi Hospital, Sharjah, UAE.
Email: ahmadsubhi73@yahoo.com
Received : Feb 10, 2026 Accepted : Mar 23, 2026 Published : Mar 30, 2026
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Subhi A © All rights are reserved
Citation: Subhi A, Alshamsi S, Al-Toubah S, Khan A, Paul A, et al. Adherence to Community-Acquired Pneumonia (CAP) management protocol among hospitalized patients: A retrospective analysis. Epidemiol Public Health. 2026; 4(2): 1095.
Abstract
Background: Community-Acquired Pneumonia (CAP) continues to be a leading hospitalization and death all over the globe, and it needs to be treated as quickly as possible, with the appropriate individual treatments and evidence-based clinical rules. Despite the widespread use of radiological imaging in the management of CAP, microbiological sampling, antibiotic choice, and duration of antibiotic therapy may be varied, as it regularly interferes with patient outcomes and antimicrobial stewardship activities.
Aims: This critique set out to measure clinical observance of diagnostic and therapeutic measures in hospitalized grown-up patients with CAP. In particular, the authors of the study compared diagnostic patterns, prescribing patterns, the overall duration of treatments, the presence of correlation between them and clinical outcomes, including mortality and complications development.
Methods: A retrospective observational audit was carried out on 221 adult patients with CAP as the first adult disease. The demographic information, radiological and microbiology studies, use of empiric antibiotics, time to treatment, and clinical outcome information were retrieved. Patient characteristics and process measures were summarized as descriptive statistics. The associations between guideline adherence and patient outcomes were also determined using chi-square analyses and the odds ratio analyses.
Results: The application of radiological imaging was almost universal, and sputum culture was carried out in only more than half of the cases. Recording of the correct initial antibiotic selection was about three fifths of the cohort, and agreement with the recommended durable antibiotic was more noticeable. There was no intriguing correlation between the appropriate selection of preliminary antibiotics and the rate of complications. Proper treatment time, however, had a considerable correlation with a high recovery rate. Admission to the ICU became a powerful prognostic indicator and the early assessment of severity needs to be realized. Detection of pathogens was not significantly related to posing risk of complications.
Conclusion: Although a high-quality performance was noted in diagnostic imaging, there are still deficiencies in microbiological testing as well as at an initial stage of antibiotic prescriptions. Durability of the use of antibiotics and proper triage by severity were closely related to good results compared to first line agent choice.
Background
Community-Acquired Pneumonia (CAP) is a significant burden to world health care, and this is because of its high rates of incidence, great morbidity and mortality, and a great cost to health care facilities. In vulnerable groups of the population, including the elderly and people with chronic conditions, CAP most frequently requires hospitalization, long-term administration of antibiotics, and, in some cases, intensive care treatment [7]. To address these issues, major institutions such as the National Institute for Health and Care Excellence [8], the European Respiratory Society [4], and BMJ Best Practice [1] have developed clinical practice guidelines that significantly promote consistent and evidence-based diagnosis and management strategies. The recommendations overlap in several key areas including: confirming the diagnosis with chest imaging, specimen collection lower respiratory tract with microbiological culture where possible, starting an empirical antibiotic regimen based on locally observed prevalence of resistance strains, and the need to keep treatment periods as short as possible, which is five to seven days in mild cases and seven to ten days in moderate to severe infection with pathogens.
Although these recommendations are supported by increasing evidence that they have a positive effect on patient outcomes, there is a lack of consistency regarding their compliance during regular patient care. A study by Costantini et al. [2] demonstrated that a higher adherence rate to guideline recommended care significantly decreased the length of stay and in-hospital deaths. A study by Fesu et al. [5] showed similar improvements in a Hungarian patient cohort after implementing structured interventions. Nevertheless, as other studies observe, such violations of recommended practice can also often correlate with the development of adverse events, the development of antimicrobial resistance, and an increased intensity of health care costs: delayed initiation of antibiotics, the inappropriate use of broad-spectrum agents, and justification of prolonged treatment regimens [3,6]. As such, a sensitive read on the local trends of guideline compliance and their association with clinical outcomes will be critical in determining quality improvement activities, including antimicrobial stewardship programs and optimal triage routes [9].
Aims/Objectives
Primary aim: Assess adherence to guideline-recommended diagnostics (sputum culture, chest imaging) and antibiotic management (initial choice, treatment duration) in adults hospitalized with CAP.
Secondary aims:
• Determine the association between adherence measures and in-hospital mortality.
• Evaluate the impact of adherence on the development of complications (e.g., empyema, respiratory failure).
• Examine the effect of admission location (ward vs. intensive care unit, ICU) on mortality and complication rates.
Methodology
Study design and setting
The present research employed a retrospective observational study design that is best suited for the investigation of the pattern of clinical practice and results during a stipulated period of history, but without affecting the pattern of physician behavior or treatment choices. The trial was carried out in a 500-bed tertiary-care teaching hospital, which acts as a regional referral facility and has all types of medical and surgical care, intensive care, and special care in relation to infectious diseases. The hospital has one of the best Electronic Medical Records (EMR) systems, and this allows for the availability of specific details of the patients uniformly throughout the hospital. The institution’s Research Ethics Committee approved the study and waived informed consent as allowed by the ethical regulations governing the carrying out of retrospective studies on anonymized data. The study was retrospective and removed any type of interaction by the patient or the clinician, and all data were de-identified before the analysis to remain confidential and versus data protection policies.
Inclusion criteria and population
Patients who were accepted to the hospital during January 1 and June 30, 2024, and with the main diagnosis of Community Acquired Pneumonia (CAP), identified based on International Classification of Diseases, 10th Revision (ICD-10) codes J13 through J18, will be included in the study population and must be adults aged 18 and older. These codes incorporate various bacterial and unspecified community-acquired pneumonias and were chosen so as to uniformly identify appropriate cases. Patients were omitted when they had a diagnosis similar to those that suggest Hospital-Acquired Pneumonia (HAP) or Ventilator-Associated Pneumonia (VAP), since both these infections are different in terms of etiology, management guidelines, and causative pathogens. Patients meeting a diagnosis alluding to Hospital-Acquired Pneumonia (HAP) or Ventilator-Induced Pneumonia (VAP) were excluded since they have distinctive etiology, management rules, and pathogens of association, evacuating patients with weakened diseases (such as the active status of chemotherapy), individuals with Human Immunodeficiency Infection (HIV) with CD4 counts less than 200 cells/mm3, as well as patients with recognized hematologic malignancies or transplant history. The cases that had incomplete or lacked information on empiric antibiotic regimens or antimicrobial therapy in all its spectrum were omitted to keep intact adherence measures and outcome comparison.
Data collection
A retrospective assessment of electronic medical records was conducted with a systematic examination administered by two infectious disease expert-trained clinicians and chart abstraction. All clinically relevant aspects of pneumonia diagnosis and treatment were captured because of the data elements selected. The demographic data, such as the age and sex of the patients, was also compiled so that the patient population could be defined and a subgroup analysis could be conducted. As diagnostic factors, there were the performance and results of the sputum cultures, the date and kind of chest radiography or computed tomography, and the radiologic results, in particular the infiltrate pattern, and their identity with the pneumonia findings. The individual recorded empiric antibiotic therapy, consisting of the type of antibiotics and dose, as well as the overall time period of the antibiotic treatment in the clinical records, was considered the therapeutic data.
The severity of illness and escalation of care in patients was best understood by classifying them based on their initial level of care upon admission, either on the general ward or in the Intensive Care Unit (ICU), as admission to the ICU typically reflects more severe presentations and influences treatment decisions made. The clinical outcomes were measured in terms of the binary outcome of in-hospital survival with or without mortality, and any complications exclusively caused by CAP, including empyema, sepsis, and Acute Respiratory Distress Syndrome (ARDS). Data abstraction was performed using a predefined extraction form, and disagreements between the two reviewers were resolved by consensus, thereby increasing the reliability of the data and reducing bias.
Statistical analysis
The statistical analysis was used to explain the patterns and analyze dependence on crucial clinical outcomes, including death and complications. The frequency of adherence and outcome variables and the characterization of the study population were done using descriptive statistics. The means of the continuous variables (e.g., patient age) were indicated along with the standard deviations to represent the central tendency and the standard deviation and categorical variables like gender, ICU admission, diagnostic adherence, and the period of treatment process were mentioned as numbers and percentages.
In search of connections between the variables of adherence and binary outcomes (mortality and complications), proportions were compared using chi-square tests across strata of adherence. In developing significant associations, Odds Ratios (ORs) were utilized against 95% Confidence Intervals (CIs) in establishing the strength and direction of the relationships. The alpha-level was 0.05 as a statistically significant result since it was based on typical hypothesis testing alpha-levels.
Results
Descriptive statistics
The cohort consisted of 221 patients, of whom 126(57.0%) were men and 95(43.0%) were women. The male preponderance of the patient population is not surprising since previous epidemiological documentation of CAP tends to show minor male predominance in hospitalizations [7]. In a huge proportion (175/221; 79.2%), cases were initially under the care of general medical wards, and 14 patients (6.3%) had to be admitted to the Intensive Care Unit (ICU) urgently. The rest (32/221; 14.5%) were probably transferred to the ICU following being admitted into a ward but are not listed separately in this group. The comparatively low episode of ICU admission with CURB-65 category indicates that the majority of the patients had mild to moderate severity of CAP (CURB-65=0-2). And a small fraction showed early stages of severe CAP that required more intense surveillance and care.
Table 1: Summary of patient characteristics, diagnostics, treatment & outcomes (n=221).
| Variable | Category | n | % |
|---|---|---|---|
| Gender | Male | 126 | 57.01% |
| Female | 95 | 42.99% | |
| Admission location | Ward | 175 | 92.59% |
| ICU | 14 | 7.41% | |
| Sputum culture done | Yes | 125 | 57.60% |
| No | 92 | 42.40% | |
| Organism found | Yes | 102 | 46.15% |
| No | 119 | 53.85% | |
| Radiology ordered | Yes | 216 | 99.08% |
| No | 2 | 0.92% | |
| Infiltrate pattern | Unilateral | 104 | 48.15% |
| Bilateral | 49 | 22.69% | |
| No infiltrate | 63 | 29.17% | |
| Correct initial antibiotic | Yes | 129 | 59.17% |
| No | 89 | 40.83% | |
| Correct antibiotic duration | Yes | 159 | 73.61% |
| No | 57 | 26.39% | |
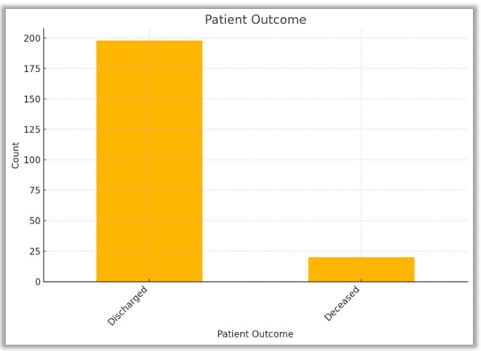
| Patient outcome | Discharged | 198 | 90.83% |
| Deceased | 20 | 9.17% | |
| Complications developed | Yes | 50 | 23.81% |
| No | 160 | 76.19% |
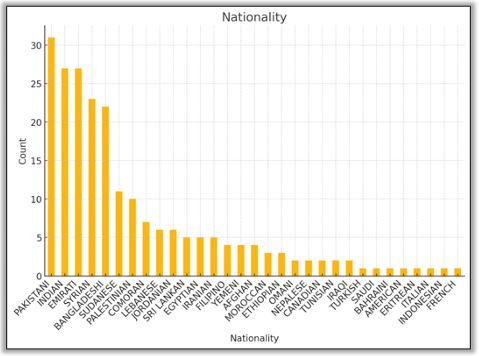
Considering the multinational character of our hospital (26 unique nationalities), it is interesting to indicate that the study population comprised 26 nationalities represented in 626\100, with the five most represented- Pakistani (31; 14.0 %), Indian (27; 12.2 %), Emirati (27; 12.2 %), Syrian (23; 10.4 %), and Bangladeshi (22; 10. Figure 1 provides a visual representation of the entire range of these nationalities, which means the variety of epidemiological backgrounds that can affect the distribution of pathogens, antimicrobial resistance tendencies, and comorbidities of patients.
Comparative analysis of diagnostics, therapeutic adherence, and outcome measures
Contrast between imaging and microbiological sampling: An enormous contrast is produced when scrutinizing the utilization of diagnostic modalities in the treatment of Community Acquired Pneumonia (CAP). An order of chest imaging, mainly through chest radiography or computed tomography, was requested in almost all the patients, 216/218 (99.08%). The reason is this near-universal dependence on imaging, which is a sign of the clinical attention given to radiologic proof of pulmonary infiltrate as an essential diagnostic feature of CAP. The logistic issues that impede the collection of samples, including the inability of patients to bring up Sputum, especially the elderly or ailing persons, tend to shorten sample collection. Second, poor quality might be an issue, which might discourage clinicians to order or process sputum cultures. There is an operational constraint, such as laboratory capacity or workflow priorities, which can help cause underutilization of culture based diagnostics. The difference visually is clear as shown in Figure 2, where the heights of Radiology Ordered bars far surpassed the heights of Sputum Culture Done bars, indicating a preference for imaging rather than microbiologic verification.
Diagnostic yield and organism detection: The 125 patients out of whom sputum cultures were successfully obtained demonstrated a pathogen in 102(81.6%) of cases, equivalent to 46.15% of the total cohort. Such a good yield in this cultured subgroup would imply that, overall, provided sputum collection is ethical and of good quality, it can provide useful etiologic information. Such limitations are the fact that they are often contaminated with oropharyngeal flora, masking actual lower respiratory pathogens, and the fact that administration of antibiotics in the pre-hospital period often alleviates microbial growth despite the presence of pathogens. The observation is consistent with the earlier findings, which have warned of the overuse of culture-negative findings in making diagnostic decisions in CAP.
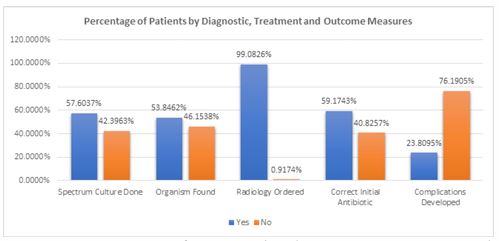
Therapeutic adherence patterns: When considering the measure of compliance with guideline-concordant therapy, there was also a significant variation in the choice of the antibiotic agent and the period of treatment. Among the 218 patients, only 129(59.17%) were provided with the NICE, ERS, and BMJ Best Practice-compatible empiric antibiotic regimens. A significantly greater fraction of the patients, however, namely 159 cases (73.61 percent), had the length of treatment in line with the recommendations: 5 7 days in case of mild and 7 10 days in case of moderate to severe pneumonia. Such a disparity suggests that antimicrobial stewardship interventions, including electronic prescribing alerts, pharmacy audits, and enforced stop orders, can be more strongly established in the long term than in the choice of the first agent. Such a difference in adherence can be a point of future efforts in providing quality improvement, striving to optimize the use of empiric therapy.
Correlation with complication rates: The possibility of association between therapeutic adherence and clinical outcomes was noted upon the comparison of complication rates. Total incidences of severe complications comprised the development of respiratory failure, empyema, or the requirement of mechanical respiration, with a total figure of 50 patients (23.81%). The figure is remarkably similar to that of the 26.39 percent (57 patients) whose antibiotic course did not comply with the guideline. This is indicative of the fact that there might be a shielding factor of the optimum duration of treatment against adverse effects. On the contrary, the absence of a significant linkage between initial non-adherence to antibiotics and complication rates suggests that these indicators of antibiotic non-adherence may not be the most important factors in defining a patient journey.
Inferential testing: Quantifying associations between ad herence and outcomes: To go beyond descriptive observations, chi-square analyses were performed, and Odds Ratios (ORs) with 95% Confidence Intervals (CIs) were calculated to deter mine key comparisons with summarized results condensed in Table 2. The analysis revealed a remarkable correlation be tween direct ICU admission and in-hospital mortality (-55.61, p< 0.001), and the OR was 54.08 (95% CI 12.97–225.56), which means that the triaged patients to the ICU at the time of admis sion experience an over-fifty-fold rise in the likelihood of dying in comparison with those admitted to ordinary wards [7].
Guideline-concordant empiric antibiotic selection has not been found to correlate with the subsequent occurrence of complications (χ²=0.42, p=0.515; OR=1.31; 95% CI 0.68–2.53) in our cohort, indicating that the empiric antibiotic regimen was perhaps not as important a determinant of short-term morbidity as the other variables such as comorbidity profiles, immune competency of the patient, and the promptness with which a strong correlation was found between following guideline recommended antibiotic ordering of duration and survival (χ²=5.06, p=0.025), with adherent patients showing a 3.17 times higher chance of being discharged alive (95% CI 1.24–8.08). The finding is consistent with the results of systematic reviews demonstrating that the correct antibiotic duration minimizes the risks of relapse and drug-related comorbidity, antibiotic resistance, and overall patient outcome [9].
Table 2: Combined inferential statistics: Chi-Square tests and odds ratio analysis.
| Comparison | Chi² | df | χ² p-value | Odds Ratio | 95% CI | OR p-value |
|---|---|---|---|---|---|---|
| ICU admission vs outcome | 55.61 | 1 | < 0.001 | 54.08 | 12.97 – 225.56 | < 0.001 |
| Correct initial antibiotic vs complications | 0.42 | 1 | 0.515 | 1.31 | 0.68 – 2.53 | 0.510 |
| Correct antibiotic duration vs outcome | 5.06 | 1 | 0.025 | 3.17 | 1.24 – 8.08 | 0.017 |
| Radiology ordered vs outcome | 0.00 | 1 | 1.000 | – | – | – |
| Organism found vs complications | 0.07 | 1 | 0.787 | 0.87 | 0.46 – 1.65 | 0.746 |
Radiology ordering, due to its almost universal usage (χ²=0.00, p=1.000), and sputum culture positivity (χ²=0.07, p=0.787; OR=0.87; 95% CI 0.46–1.65) did not show any significant association with mortality or complication rates either. The null results can probably be attributed to underwhelming variability in the radiology ordering and moderate sensitivity of the sputum cultures and a slowness in the reporting of cultures that severely reduce their influence on the immediate clinical decision-making [1,3].
Conclusion
When we go through our analysis of community-acquired pneumonia management at one of the hospitals providing tertiary care, the following themes can be identified that can be viewed as higher-level metrics indicative of the overall quality of care. On the one hand, the almost unanimous adoption of chest imaging supports the extent of the awareness by the clinics of the importance of radiographic confirmation of the ultimate disease diagnosis and the stratification of the disease severity. The robust performance enables it to be built upon the development of more discriminating plays of diagnosis, especially those that help with quick, definitive identification of the pathogen and thus guide more specific antibiotic selection.
The adoption of microbiological sampling was not so consistent, however, indicating a major area needing improvement in the manufacturing process, especially when it came to sputum collection and lab operations. The optimization of pathogen-directed therapy response may be achieved by streamlining specimen collection, accelerating the processing, and enabling healthcare teams to enhance the yield, minimize the utilization of broad-spectrum empiric regimens, and, eventually, facilitate the more responsible application of antibiotics.
We also emphasized the implication of antimicrobial stewardship approaches that should not be limited to the selection of the initial agent but should be applied throughout the treatment period. Specifically, formal systems to repeat and withdraw treatment at guideline-suggested intervals seem to be relevant to prescribers more robustly than are initial agent algorithms. Training programs, audits by pharmacies, and electronic reminders about best practice can be integrated into clinical workflows to reinforce best practice and make sure that patients are not prescribed too much or too little, antibiotic therapy.
The most dramatic evidence, perhaps, is that the prognosis can be altered significantly by identifying disease severity and properly elevating care at an early stage. Whether using formality severity-scoring instruments or triage pathways covering a wide range of specialists, the capability to distinguish among individuals at greatest risk and the capacity to mobilize intensive resources with dispatch will be a key component of success in pneumonia management. An investment made in the area of education, decision-support systems, and interprofessional collaboration concerning the area of severity assessment will be repaid through better outcomes of patient care and the use of resources.
References
- BMJ Best Practice. Community-acquired pneumonia in adults: investigations. 2024.
- Costantini E, Allara E, Patrucco F, Faggiano F, Hamid F, Balbo PE. Adherence to guidelines for hospitalized community-acquired pneumonia over time and its impact on health outcomes and mortality. Intern Emerg Med. 2016; 11: 929-940.
- Eccles S, Pincus C, Higgins B, Woodhead M. Diagnosis and management of community and hospital acquired pneumonia in adults: summary of NICE guidance. BMJ. 2014; 349: g6722.
- European Respiratory Society (ERS). Community acquired pneumonia: what’s new with 2024 recommendations. 2024.
- Fésüs A, Benkő R, Matuz M, Engi Z, Ruzsa R, Hambalek H, et al. Impact of guideline adherence on outcomes in patients hospitalized with community-acquired pneumonia (CAP) in Hungary: a retrospective observational study. Antibiotics (Basel). 2022; 11: 468.
- Han X, Zhou F, Li H, Xing X, Chen L, Wang Y, et al. Effects of age, comorbidity and adherence to current antimicrobial guidelines on mortality in hospitalized elderly patients with community-acquired pneumonia. BMC Infect Dis. 2018; 18: 192.
- Modi AR, Kovacs CS. Community-acquired pneumonia: strategies for triage and treatment. Cleve Clin J Med. 2020; 87: 145-151.
- National Institute for Health and Care Excellence (NICE). Pneumonia (community-acquired): antimicrobial prescribing. 2019.
- Seo C, Corrado M, Lim R, Thornton CS. Guideline-concordant therapy for community-acquired pneumonia in the hospitalized population: a systematic review and meta-analysis. Open Forum Infect Dis. 2024; 11: ofae336.
- Waagsbø B, Tranung M, Damås JK, Heggelund L. Antimicrobial therapy of community-acquired pneumonia during stewardship efforts and a coronavirus pandemic: an observational study. BMC Pulm Med. 2022; 22: 343.