
Research ArticleOpen Access, Volume 4 Issue 2
Persistent disparities in the modern era of brain metastasis treatment: A SEER-based Study (2010–2022)
Daniel Holguin*; Oluwasegun Akinyemi, PhD; Noor Malik, MD
Howard University Hospital, Washington, DC, USA.
*Corresponding author: Daniel Holguin
Howard University Hospital, Washington, DC, USA.
Email: daniel.holguin@bison.howard.edu
Received : Mar 02, 2026 Accepted : Apr 08, 2026 Published : Apr 15, 2026
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Holguin D © All rights are reserved
Citation: Holguin D, Akinyemi O, Malik N. Persistent disparities in the modern era of brain metastasis treatment: A SEER-based Study (2010-2022). Epidemiol Public Health. 2026; 4(2): 1096.
Abstract
Background: Metastatic Brain Tumors (MBTs) are more common than primary brain tumors and associated with poor survival. This study examined whether race × income interaction predicts differences in treatment receipt and survival among patients with MBTs from lung, breast, melanoma, and prostate cancer.
Methods: We analyzed SEER data from 2010-2022, identifying adults with MBTs from lung, melanoma, breast, and prostate primaries. Treatment outcomes included receipt of chemotherapy, radiation, or surgery, and the sequence of radiation or chemotherapy relative to surgery. Survival outcomes were modeled using Cox proportional hazards regression. Unadjusted, adjusted, and interaction models (race and income) were run separately for each cancer type. Income was binarized into low and high using a cutoff of $75,000.
Results: A total of 77,895 patients were included (69,928 lung, 3,786 melanomas, 3,588 breast, 593 prostate). Mean age was 65 years (SD 5 years), 71% were White, and 40% fell into the low-income category. In the adjusted survival model, Hispanic and Asian lung cancer patients showed improved survival compared to White patients (HR 0.93 and 0.71, CI 0.93-0.96 and 0.68-0.72, respectively, p<.001), while low-income patients had worse outcomes (HR 1.66, CI 1.14 1.18, p<.001). After interaction modeling, low-income Black patients with lung cancer had a survival advantage over low-income White patients (HR 0.92, CI 0.87-0.97, p=.001), while Asian and Hispanic patients maintained their survival advantage regardless of income. Black patients with breast MBTs experienced persistently worse survival, regardless of model (HR 1.19, CI 1.02-1.38, p=.019).
Conclusion: Income modifies the effect of race on survival in patients with MBTs, challenging past assumptions that race alone predicts poorer outcomes. Findings suggest that survival disparities may be driven more by socioeconomic conditions than differential treatment access.
Keywords: Brain metastases; SEER database; Neuro-oncology; Survival analysis; Health disparities.
Introduction
Metastatic Brain Tumors (MBTs) are four times more common than primary brain tumors [1]. Despite therapeutic advances, their diagnosis confers an average survival of less than one year [2]. Among MBTs, some of the most common primary sources of metastases include lung, breast, melanoma, and prostate. Previous studies using data from the Surveillance, Epidemiology, and End Results database (SEER) have described disparities in treatment and survival by race and socioeconomic status in each of these cancer types [3-6]. However, these studies have not incorporated interaction models to assess how these variables interact.
The past two decades have seen rapid evolution in MBT management with the advent of Stereotactic Radio Surgery (SRS) and targeted immunotherapies [7]. Recent studies have started to examine whether racial and economic disparities in access to these treatments have contributed to persistent survival gaps. For example, rural patients—who are further from academic centers—are less likely to receive advanced MBT directed therapies, which are associated with worse survival [8]. Historically, Black patients with MBTs have had lower overall survival compared to White patients. However, a recent SEER study using data from 2010-2019 found that after controlling for socioeconomic status, survival outcomes were improved among all minority patients compared to Whites [2,9]. Notably, this study did not use an interaction model between race and income to further investigate these findings.
This study tests an interaction model between race and income using SEER data from 2010-2022, with a focus on MBTs from breast, prostate, lung, and melanoma cancers. In addition to survival analyses, we examined disparities in treatment receipt and sequence.
Methods
Data source and cohort selection: Data was compiled from the SEER Research database. The name of the database within SEER used to retrieve case files was “Incidence – SEER Research Data, 17 registries, Nov 2024 Sub (2000-2022)”; SEER Research Plus and SEER-Medicaid data was not available for this analysis. Patients were ≥18 years old and had evidence of brain metastases at diagnosis (filtered using “SEER Combined Mets at DX-brain”). The primary cancer sites were filtered by “ICD-O-3/WHO 2008” and included prostate, lung, breast, and melanoma. Cases ranged from 2010 to 2022. This study was approved with expedited review by the Howard University IRB. All data preprocessing, variable recoding, modeling, and output formatting were conducted using R version 4.5.
Variable selection and classification
Demographic and clinical variables were used for analyses. Race was derived from “Race and origin recode (NHW, NHB, NHAIAN, NHAPI, Hispanic (All Races))”, which was simplified to White, Black, American Indian and Alaskan Native, Asian and Pacific Islander, and Hispanic. Economic status was derived from “Median household income inflation adj to 2023” and split into low (<$75,000) or high ($≥75,000) income as opposed to quartiles in the interest of preserving variance for our regression analyses. Rural-urban status was based on the “Rural-Urban Continuum Code,” dichotomized as Urban or Rural. Age at diagnosis was parsed from the variable “Age recode with single ages and 90+” and converted into a numeric variable. “Year of diagnosis” was split 2010-2014 and 2015-2022 to reflect changes in treatment guidelines, referred to in this analysis as diagnosis era. Extent of disease was controlled for using the variable “First malignant primary indicator” (yes or no).
Binary variables were created to determine whether cases received chemo, radiation, surgery, or any combination of all three using “Chemotherapy recode (yes, no/unk)”, “Radiation recode”, “RX Summ-Surg/Rad Seq”, and “RX Summ-Systemic/ Sur Seq (2007+)”. The sequence of radiation or chemo in reference to surgery was derived from “RX Summ-Surg/Rad Seq” and “RX Summ-Systemic/Sur Seq (2007+)”.
Survival variables included “Survival months”, “COD to site recode ICD-O-3 2023 Revision” (cause of death), and “Vital status recode (study cutoff used)”.
Treatment and survival analysis
We evaluated three primary outcomes: receipt of treatment modalities (surgery, chemotherapy, radiation, or any combination), treatment sequence (whether chemotherapy or radiation occurred before, after, or both before and after surgery), and survival outcomes (overall and 5-year survival). For each outcome, we conducted a series of logistic or Cox regression models in three tiers: unadjusted, adjusted, and interaction models testing for race × income effects.
Binary logistic regressions were used for all treatment receipt and treatment sequence outcomes. Control group included White race, income ≥$75k, married, “first primary tumor” = Yes, and “Number of In Situ/Malignant Tumors” = 1. Adjusted models controlled for age, sex (except for prostate), race, income, marital status, rural vs. urban residence, diagnosis era, tumor count, first primary status, and time from diagnosis to treatment. Due to insufficient variance, treatment sequence outcomes were modeled using binary regressions only; multinomial regression was not feasible. These sequence variables were not included as predictors in survival models.
Time-to-event outcomes were assessed using Cox proportional hazards regression to estimate overall survival (in months) with right-censoring of patients alive at last follow up. Binary 5-year survival was modeled separately. Cox models were stratified by cancer type and included the same covariates and interaction terms as the logistic models.
Results
Descriptive statistics and common findings across cancer types
Descriptive statistics of each cohort are summarized in (Table 1). The total number of patients was 77,895. The overall mean age was approximately 65 years. Approximately 40% of patients fell into the low-income group (household income <$75,000), and 71.5% resided in urban areas. The average time between diagnosis and treatment was 21 days overall. Mean survival across the cohort was approximately 15 months.
Across all four cancers, older age, extended time between diagnosis and treatment, non-married status, and prior malignancies were consistently associated with lower odds of receiving treatment and lower survival.
Given the large volume of data generated from the analysis, we decided to limit the results of this paper to the interaction model and focus on race and income differences. Other notable findings will be mentioned briefly below and explored in a subsequent report.
Table 1: Cohort summary.
Differences in treatments received
The results of the race and income interaction on receipt of treatment are illustrated collectively and by cancer type in (Figure 1).
Lung: In the interaction analysis of race and income, American Indian/Alaska Native (AIAN) patients with incomes ≥$75,000 were less likely to receive systemic therapy compared to low- or high-income White patients (OR 0.65, CI 0.46-0.93, p=0.018), while those with incomes <$75,000 were less likely to receive all three treatments (OR 0.54, CI 0.30-0.96, p=0.034). Asian/Pacific Islander (API) patients with high income were more likely to receive systemic therapy (OR 1.54, CI 1.42-1.66, p< 0.001) but less likely to receive radiation, surgery, or all three treatments. Black patients with low income were less likely to receive systemic therapy (OR 0.68, CI 0.63-0.73, p<0.001) and all three treatments (OR 0.85, CI 0.76-0.94, p=0.001), but more likely to receive chemotherapy (OR 1.23, CI 1.11-1.37, p<0.001). Black patients with high income were less likely to receive chemotherapy (OR 0.75, CI 0.69-0.81, p<0.001) or all three treatments (OR 0.89, CI 0.79-0.99, p=0.040). Hispanic patients, regardless of income level, had lower odds of receiving all forms of treatment (high income: OR 0.78, CI 0.69-0.88, p<0.001; low income: OR 0.76, CI 0.63-0.90, p=0.002). Among White patients, those with low income were significantly less likely to receive all forms of treatment (OR 0.91, CI 0.86-0.97, p=0.005). Diagnosis between 2010-2014 was associated with lower odds of receiving all three treatments (OR 0.84, CI 0.80 0.89, p<0.001) but higher odds of receiving radiation (OR 1.39, CI 1.32-1.46, p<0.001).
Melanoma: High-income Hispanic patients were less likely to receive radiation (OR 0.64, CI 0.42–0.98, p=0.030), while low-income White patients were more likely to receive all three treatments compared to high-income Whites (OR 1.36, CI 1.03 1.78, p=0.020). Diagnosis during 2010-2014 was associated with increased odds of receiving all treatments (OR 2.58, CI 2.03 3.29, p<0.001). Divorced and single patients were less likely to receive systemic therapy (OR 0.71, CI 0.52-0.96, p<0.001; OR 0.76, CI 0.61-0.96, p<0.001, respectively).
Breast: Low-income Hispanic patients were less likely to receive radiation (OR 0.61, CI 0.41-0.90, p=0.010), while low income Black patients were less likely to receive systemic therapy (OR 0.72, CI 0.53-0.99, p=0.040). Patients diagnosed between 2010-2014 were also less likely to receive systemic therapy (OR 0.67, CI 0.56-0.80, p<0.010). All non-married statuses—single, separated, divorced, and widowed—were associated with decreased odds of receiving all treatments.
Prostate: In the interaction model, high-income Hispanic patients were significantly less likely to receive systemic therapy compared to high-income White patients (OR 0.36, CI 0.15-0.86, p=0.020). Patients diagnosed during 2010-2014 had lower odds of receiving systemic therapy (OR 0.52, CI 0.29-0.91, p=0.020). Separated and single patients were significantly less likely to receive all forms of treatment.

Treatment sequence differences
The interaction analysis of race and ethnicity on treatment sequence was less revealing than the treatment type models. The number of possible outcomes was more than double in some datasets, leading to a reduced number of patients in each outcome, and less statistical power. Significant findings are included below and in (Table 2).
Lung: patients with income <$75,000 were significantly less likely to receive systemic therapy after surgery than other races at the same income level (OR 0.39, CI 0.24-0.64, p<0.001). They were also less likely to receive intraoperative systemic therapy (OR 0.37, CI 0.23-0.58, p<.001).
Black patients with income <$75,000 were more likely not to receive systemic therapy and/or surgical procedures overall (OR 6.35, CI 4.20-9.58, p<.001), but also more likely to receive intraoperative systemic therapy (OR 17.14, CI 8.54-34.39, p<.001).
Melanoma: Black patients, regardless of income, were less likely to receive surgery both before and after radiation (OR 0.45, CI 0.44-0.45, p <.001). This finding was also found in the other models. While other findings reached significance, the results suggested a lack of variance in the subgroups created, resulting in large confidence intervals and unreliable estimates.
Breast: In the interaction model, patients with income <$75,000 were more likely not to receive systemic therapy and/ or surgery (OR 3.68, CI 2.51-5.39, p<0.001) but more likely to receive systemic therapy before and after surgery (OR 2.96, CI 1.43-6.11, p<.005). Similar to the melanoma cohort, other significant findings were limited by large confidence intervals.
Prostate: Black patients with income <$75,000 were less likely to receive systemic therapy before surgery (OR 0.08, CI 0.03-0.29, p<0.001), while Hispanic patients appeared less likely to receive systemic therapy after surgery (OR 0.24, CI 0.08-0.74, p=0.01), in the interaction model. Similar associations were also found in the non-interaction models.
Survival analysis
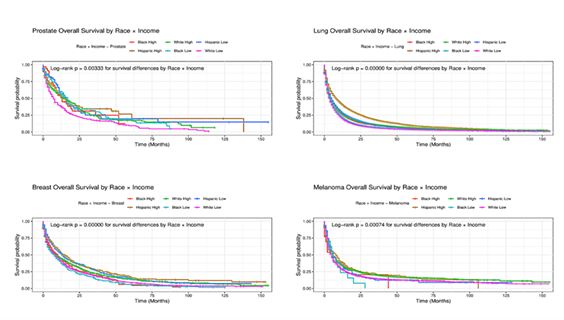
Significant interaction findings for race and income on survival are illustrated in (Figure 2).
Lung: In the adjusted survival model, Hispanic and Asian lung cancer patients showed improved survival compared to White patients (HR 0.93 and 0.71, CI 0.93-0.96 and 0.68-0.72, respectively, p<.001), while low-income patients had worse outcomes (HR 1.66, CI 1.14-1.18, p<.001). After interaction modeling, low-income Black patients with lung cancer had a survival advantage over low-income White patients (HR 0.92, CI 0.87-0.97, p=.001), while the associations found earlier in Asian and Hispanic patients remained consistent regardless of income.
Other significant findings included: increased risk for rural patients (HR 1.06, CI 1.03-1.09, p<.001), males (HR 1.24, CI 1.22 1.26, p<.001), and non-married patients (HR 1.25, CI 1.23-1.27, p<.001), as well as those diagnosed in 2010-2014 compared to 2015-2022 (HR 1.28, CI 1.26-1.30, p<.001).
Melanoma: The interaction model did not find significant differences by race but income, regardless of race, showed increased risk (HR 1.13, CI 1.04-1.24, p=0.004), this finding was also found in the other models. Non-married patients and those diagnosed between 2010-2014 also had increased risk (HR 1.22 and 1.33, CI 1.13-1.32 and 1.23-1.44, p<0.001, respectively).
Breast: Black patients with breast MBTs experienced persistently worse survival, regardless of model (HR 1.19, CI 1.02-1.38, p = 0.019). Low-income patients in general and men also had increased risk: HR 1.14 and 1.56, CI 1.03-1.27 and 1.12 2.17, p=0.013 and 0.008, respectively.
Prostate: In the unadjusted model Hispanic patients showed increased survival, HR 0.61, CI 0.45-0.82, p=0.001. This finding was significant after adjusting for cofounders but not after controlling for race x income interaction.
In the interaction model, the HR for AIAN patients, regardless of income, was 20.27, but the confidence interval introduced uncertainty in its’ significance, CI 2.76-148.89 (p=.003), due to small sample size. Non-married patients also showed increased risk (HR 1.29, CI 1.06-1.57, p=0.01).
Table 2: Interaction of race and income level on odds of receiving treatment sequence.
Discussion/Conclusion
This study is the first, to our knowledge, to use a race × income interaction model in a SEER-based analysis of treatment receipt, treatment sequencing, and survival among patients with metastatic brain tumors from lung, breast, melanoma, and prostate primaries. By stratifying analyses by cancer type and examining how race and income jointly influence outcomes, we found that income substantially modifies the effect of race on both treatment patterns and survival. In lung cancer, for example, low-income Black patients had a survival advantage over low income White patients despite receiving fewer multimodal treatments, while Hispanic and Asian patients-maintained survival advantages, regardless of income. Conversely, breast cancer MBTs demonstrated persistently worse survival for Black patients in all models, suggesting that some disparities remain independent of income. Our results also show that treatment sequencing disparities were less consistent and often limited by small sample sizes, highlighting the need for more granular data in this domain.
A major strength of this study is its novel methodological approach, using interaction modeling to uncover disparities that would be obscured in main-effects-only models. By focusing on MBTs diagnosed between 2010-2022, we captured an era of rapid therapeutic innovation, including broader adoption of stereotactic radiosurgery and targeted systemic therapies. Our stratified cancer-type analysis also provides clinically relevant insights for tumor-specific care pathways. However, several limitations warrant discussion. First, SEER lacks detailed clinical variables such as insurance information and molecular profiles, which may confound observed associations. Second, treatment variables do not differentiate between contemporary modalities (e.g., SRS vs. whole brain radiotherapy) or novel systemic agents, limiting specificity. Third, the rarity of certain treatment sequences, particularly intraoperative therapy, led to unstable estimates with wide confidence intervals in some subgroups. Finally, income was measured ecologically at the county level and may not reflect individual patient circumstances, potentially introducing misclassification bias.
Our findings suggest that socioeconomic context modifies racial disparities in MBT outcomes, challenging the historical assumption that race alone drives poorer survival. The improved survival among low-income Black patients with lung MBTs compared to their White counterparts, as well as the persistence of survival advantages in Asian and Hispanic groups, raises important questions about unmeasured factors such as differential tumor biology, healthcare-seeking behavior, or treatment tolerability. The persistently worse survival among Black breast cancer patients across income strata points to disease-specific disparities that may not be mitigated solely by socioeconomic interventions. The observed treatment differences, including reduced odds of multimodal therapy in certain racial-income groups, underscore the importance of equitable treatment access in translating advances in MBT care into survival gains.
Future research should integrate more granular clinical, molecular, and treatment delivery data to better elucidate the drivers of these disparities. Linkage of SEER data to claims databases or institutional registries could clarify the role of advanced modalities such as SRS, immunotherapy, and targeted agents in modifying survival. Prospective studies are also needed to evaluate whether targeted interventions—such as patient navigation programs or improved access to specialized neuro-oncology care—can reduce disparities identified in this analysis. Finally, as therapeutic innovation continues, ongoing surveillance of equity in MBT care should remain a priority to ensure that emerging treatments narrow, rather than widen, existing gaps in outcomes.
References
- Bertolini F, Spallanzani A, Fontana A, Depenni R, Luppi G. Brain metastases: an overview. Cancers (Basel). 2019; 11: E29.
- Jiang SH, Bhaskara M, Deysher D, et al. Racial disparities in incidence, treatment, and survival in adult brain metastases: a 10-year national database analysis. Neurosurg Focus. 2023; 55: E6.
- Al Rifai M, Alruwaili M, Khan R, et al. Disparities in the use of radiotherapy for brain metastases from lung cancer. Cureus. 2021; 13: e16477.
- Moore JX, Andrzejak SE, Han Y, et al. Exploring the intersectionality of race/ethnicity with rurality on breast cancer outcomes: SEER analysis, 2000–2016. Breast Cancer Res Treat. 2022; 192: 569–579.
- Schwartz K, Powell IJ, Underwood W III, George J, Yee C, Banerjee M. Interplay of race, socioeconomic status and treatment on survival of prostate cancer patients. Urology. 2009; 74: 1296–1302.
- Qian Y, Johannet P, Sawyers A, Yu J, Osman I, Zhong J. Ongoing racial disparities in melanoma: an analysis of the SEER database (1975–2016). J Am Acad Dermatol. 2020; 83: 955–957.
- Vogelbaum MA, Brown PD, Messersmith H, et al. Treatment for brain metastases: ASCO-SNO-ASTRO guideline. J Clin Oncol. 2022; 40: 492–516.
- Riggs J, Ahn H, Longmoore H, et al. Addressing disparities in delivery of cancer care for patients with melanoma brain metastases. Neurooncol Adv. 2023; 5: vdad113.
- McCray E, Waguia R, de la Garza Ramos R, et al. Racial disparities in inpatient clinical presentation, treatment, and outcomes in brain metastasis. Neurooncol Pract. 2023; 10: 62–70.